ADHD
Summer 2026
HIGHLIGHTS
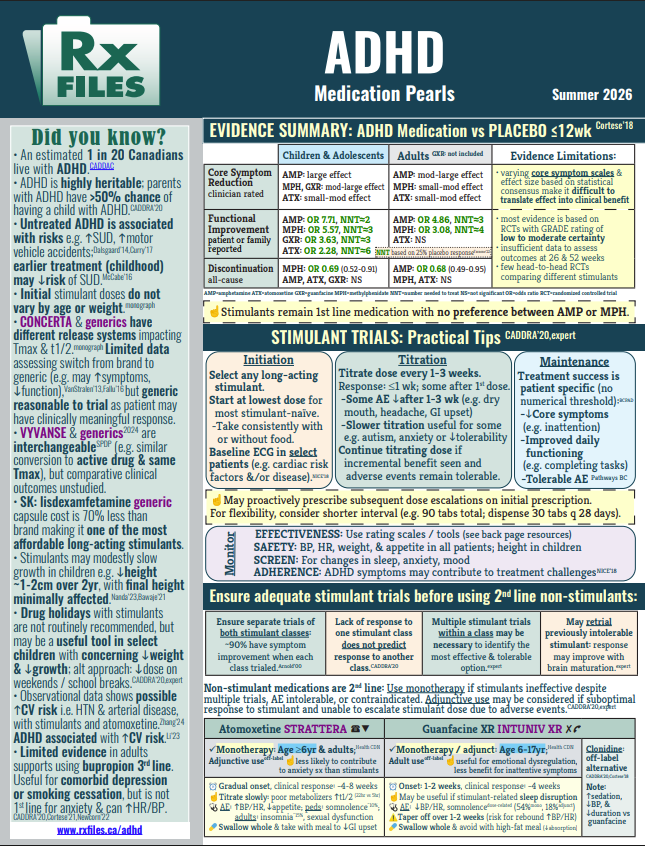
· Practical clinical pearls to support individualized stimulant selection based on medication characteristics and patient-specific factors.
· Initiating stimulant therapy, optimizing titration and monitoring, and ensuring an adequate therapeutic trial.
· Practical strategies for managing common challenges encountered when adjusting stimulant therapy.
· When to consider second-line non-stimulant options following multiple stimulant failures.
Visit: www.rxfiles.ca/adhd